
How PHIL is Rewriting the Rules of Direct-to-Patient

“When you build a DTP program designed for patients, with affordable and transparent pricing, coverage options, and real-time support, access and adherence outcomes amplify.”
Pharmaceutical companies spend years and billions of dollars developing branded therapeutics. They navigate clinical trials, regulatory review, and market access negotiations to get a product to market. And then, at the very last step, the system that is supposed to connect a therapy to the patient who needs it often fails to do so.
Not because patients don’t want to take their medication. Because the infrastructure designed to deliver it was never built with the patient in mind.
Here is a scenario: A patient leaves a doctor’s office with a prescription and a list of next steps, but no one has time to help them navigate them. They arrive at a pharmacy counter and encounter a price they didn’t anticipate, with no context, no options, and no clear path to a better outcome. They may not know that coverage could significantly reduce that cost, that a prior authorization is holding things up, or that there is any recourse at all. So they either walk away or fill once and stop when the cost doesn’t improve.
This is the structural problem that Direct-to-Patient programs are being built to address, and it is the problem that PHIL has spent more than a decade working on, before the field even had a name for it.
“That same concept was there from the beginning,” said Josh Zeidman, SVP, Business Development at PHIL. “A patient is a consumer, and you need to engage them and educate them and provide them with something they enjoy using if they’re going to successfully obtain their medication and stick to it.”
Where pharma DTP programs stand today
The DTP landscape is not uniform. When PHIL looks at its pharma partners, Zeidman describes three distinct archetypes, each at a different stage of the journey.
The first group includes brands with established DTP programs, many of which have been building for two or more years. They have ecosystems in place, but the ecosystems have gaps. Coverage depth, adherence support, and patient experience consistency are common shortfalls. The second group is moving fast, looking to get into the market quickly and start learning. They need a partner who can help them stand something up without sacrificing quality. The third group is moving deliberately, often for a new product launch, co-designing something customized from the ground up.
PHIL works across all three. What changes is the kind of partnership required.
For the first group, PHIL often fills specific gaps in an existing program, adding hybrid cash and coverage pathways, strengthening refill processes, or improving a disjointed patient experience. For the second, speed and best-practice knowledge are the primary contributions. For the third, PHIL functions as a strategic program design partner, working directly with the pharma team to map out strategy, pilot different approaches, and refine based on what the data shows.
“We are definitely not a one-size-fits-all company,” Zeidman said. “We understand that all brands have unique needs, goals, and priorities, even when under the same manufacturer. We’ll sit down with the brand team, and we’ll build a custom program design for their specific product — we’ll lay out the different strategies for how they can enter the market or scale existing DTP programs to make them a better experience.”

Built for what patients are seeking
PHIL recently surveyed over 1,000 patients about their prescription access experience, and the results were, in Zeidman’s words, “almost intuitive.” Patients want to access their medications through their preferred channel, whether online, in person, or a combination of both. They want price transparency. They want to know what they’ll pay before they stand at the counter. They want affordability. And they want an experience that mirrors what they already know and expect from e-commerce.
This last point is not incidental. PHIL’s Founder & CEO, Deepak Thomas, comes from an e-commerce background, and those principles have shaped how the platform is built and continues to evolve. The patient-facing experience draws on what companies like Amazon have spent decades learning about how consumers engage online.
The contrast with the traditional pharmacy experience is stark. Right now, most patients arrive at a counter and are presented with a price they may not anticipate, without context, without options, without any clear way to know if they’re getting the best price available to them. They may go home and search for coupons, return to the pharmacy, and hand over a printed coupon after already making multiple trips. Each of those friction points is a potential exit from therapy.
“It’s a black-box experience,” Zeidman said. “As the patient, you don’t know what your options are. As the manufacturer, you don’t know what’s going on for patients and where preventable friction may be occuring.”
PHIL’s platform replaces that experience with a guided prescription access journey with transparent pricing, multiple access pathways, and the work of navigating coverage handled on the patient’s behalf.
The case for coverage as part of DTP
One of PHIL’s most important contributions to how the industry thinks about DTP is pushing back on the assumption that Direct-to-Patient is synonymous with cash pricing.
Cash prices have grown in popularity and, in some cases, have genuinely lowered costs for patients. But cash is not the right answer for every patient or product. For many, insurance coverage, despite the complexity it can introduce, will result in a lower out-of-pocket cost than a cash price. A $20 copay and a $100 cash price are not equivalent options, but without someone navigating coverage on the patient’s behalf, the faster, simpler cash path tends to win by default.
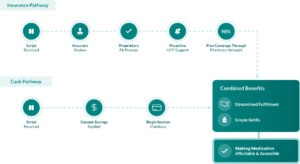
PHIL Direct is designed around the patient, equipping manufacturers with cash, coverage, and hybrid program flexibility. In the coverage and hybrid route, when a patient enters the platform, PHIL checks for insurance status, runs a coverage claim if applicable, and supports technology-enabled prior authorizations where required. The goal is to get each patient to the lowest cost available to them through their desired pathway, not just the most expedient one.
“In everything we do, we want to lead with doing what’s right for the patient,” Zeidman said. “We help manufacturers operationalize the ideal approach that makes most sense for their patients.”
Brands that invest in co-pay programs and coverage support often see that investment undermined when patients default to cash out of confusion rather than by choice. PHIL’s flexible DTP model ensures that coverage infrastructure can be part of the DTP equation.
The data layer
A key differentiator that distinguishes PHIL’s platform from point solutions is the holistic, granular data generated for pharma teams. As PHIL manages the patient relationship from initial contact through dispense and refill, it captures an end-to-end record of the patient journey that stitched-together or disjointed data systems simply cannot produce.
Zeidman describes the challenge facing most pharma partners today: when multiple vendors handle different parts of the process, patient-level data gets fragmented. Protected health information rules make it difficult to connect what happened at one handoff point to what happened at another. The full picture of why a patient dropped off, where in the journey it happened, and what might have changed the outcome is often impossible to reconstruct.
PHIL’s architecture eliminates data fragmentation. Because the platform is shepherding the patient from start to finish, it captures everything. The brand team has visibility into where a patient came from, whether they book and complete an appointment, fill and refill a prescription, and where drop-off occurs. That integrated insight about the journey creates an opportunity for brands to optimize their program structure proactively before drop-off occurs.
“For pharma leaders, this data is a complete game-changer. Brand teams can actually solve the problem upstream through equipping patients with an optimized journey upfront based on the data they’re seeing in real-time.” ” Zeidman said.
The data is surfaced in live dashboards and real-time feeds that pharma partners can access directly, rather than waiting for periodic data exports that are always looking backward. Field teams can also act on current information with script-level and prescriber-level insights. Program managers can see where prior authorizations are creating backlogs and address them. The data becomes a strategic tool for ongoing, proactive brand management rather than a historical record.

Increasingly, PHIL is layering AI within their data infrastructure, allowing partners to query patient trends and surface insights without manual analysis.
“You can talk to an AI model and say, based on the data I’m seeing, what trends are we observing,” Zeidman said, “and all of a sudden you can get instant feedback without having to do a bunch of manual data work yourself.”
What better looks like
The outcomes PHIL has documented across its pharma partner programs are worth highlighting directly. Refill rates have increased by more than three times compared to traditional channels. Coverage rates, measuring how many new prescriptions written actually result in a dispensed, covered fill, have more than doubled.
Those numbers carry weight because of where they sit in the drug development timeline. By the time a patient has a prescription in hand, a pharmaceutical company has already made its largest investment. Clinical development, regulatory approval, and market access work are behind it. What remains is the question of whether patients actually start and stay on their prescribed medication, which is critical to driving positive therapy outcomes. And the data suggests that, without deliberate infrastructure supporting this essential step, a significant share of patients do not.
Access, affordability, and adherence are not independent variables. They compound. More patients on covered pathways means lower out-of-pocket costs, which means more refills, which means more patients seeing clinical benefit. Each improvement multiplies the others.
The work still ahead
Zeidman is clear about where the field still has room to grow. The most common limitation he sees is scope. Direct-to-Patient is too often treated as a cash-price program, a single discounted pathway for a specific subset of patients. That framing leaves a lot of potential on the table.
“I think there’s a common notion in the industry today that Direct-to-Patient is essentially a ‘cash price with a coupon’ program,” he said. “That’s a good way to start thinking about it, but these programs have the potential to be so much more than that.”
“For pharma brands preparing to launch or optimize a DTP program today, the better question is how can DTP function as a full access strategy,” Zeidman said.“Cash for some patients, coverage support for others, education and engagement for everyone, all coordinated through a single platform that offers flexibility as the market evolves.”
A shared framework for the industry
PHIL’s participation in DiMe’s Direct-to-Patient project is oriented around exactly this kind of strategic, industry-level thinking. The DTP field is at an early enough stage where foundational frameworks still matter, and building shared language and best practices around what DTP should include, beyond cash or a single channel, across the full arc of the patient journey, will shape how pharma brands invest and how patients ultimately experience their care.
Zeidman put it perfectly: “If people start thinking about DTP as a strategic framework, the industry will evolve and uplevel into the next generation of patient centricity and experience.” .”
This clarity is what DiMe is working toward alongside partners like PHIL, and the evidence is accumulating that when pharma companies get the DTP model right, the results show up where it matters most: more patients getting the medications they need, staying on them, and benefiting from them.
Discover the DTP possibilities with PHIL Direct, learn more at phil.us.

