Evidence in Digital Health for EFfectiveness of INterventions with Evaluative Depth (Evidence DEFINED)
The new standard of excellence framework for clinical assessment of digital health products (DHPs).
Quick Start Guide
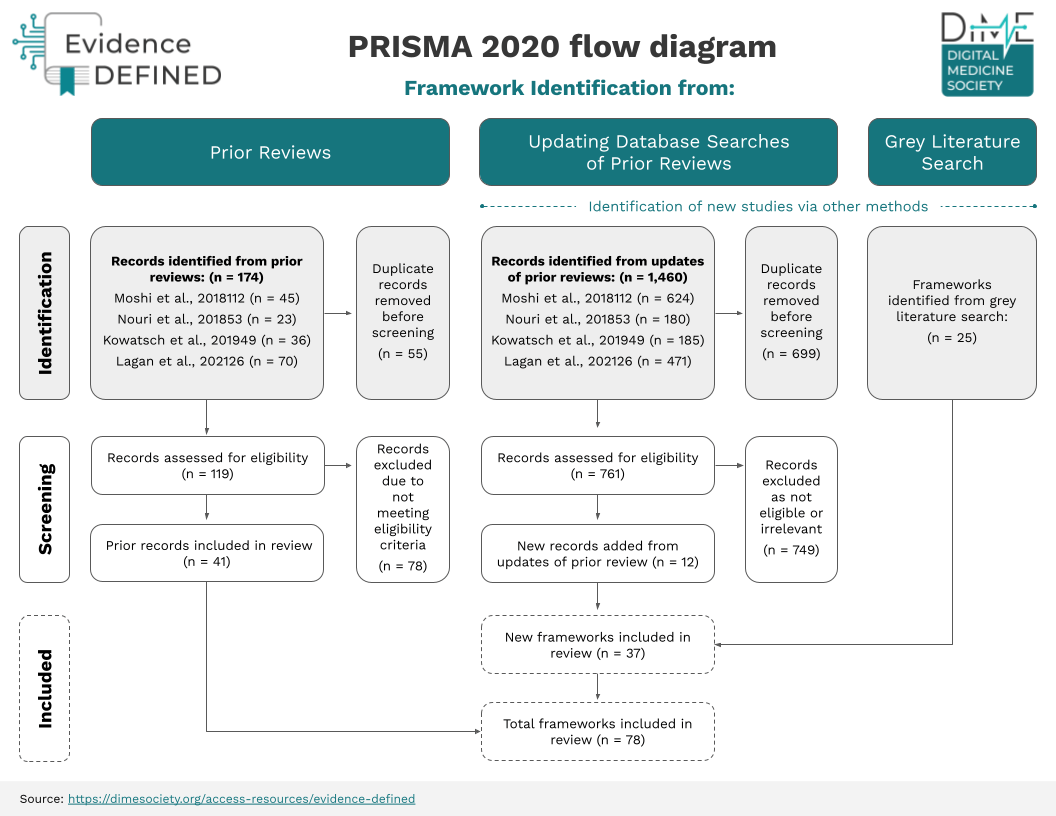
A process overview for the Evidence DEFINED Framework

Download or share this resource:
Download or share this Resource:

Download or share this Resource:
Catch the replay!
Watch as the co-authors showcased and discussed Evidence DEFINED during a DiMe Journal Club. Tune into the recording or access the presentation slides.
In this journal club, the co-authors came together to showcase the framework, which offers payers, employers, health systems, and other users a harmonized, rigorous, rapid approach to assessing the clinical value of DHPs and bringing them to market faster.

If you would like to engage in DiMe’s upcoming IEP project and help streamline the path to regulatory and commercial success to optimize health outcomes for the greatest number of patients, learn more and share your interest to join:

