
DiMe Webinar Series recently addressed the topic of women’s experience with digital health. While digital health technologies (DHTs) have come a long way, many commercially available health and wellness tools are not designed to be inclusive of the experiences and needs unique to women. The webinar explored personal use cases and design & development expert opinions on how currently available tools can be used within this space.
Personal experience – pregnancy and motherhood
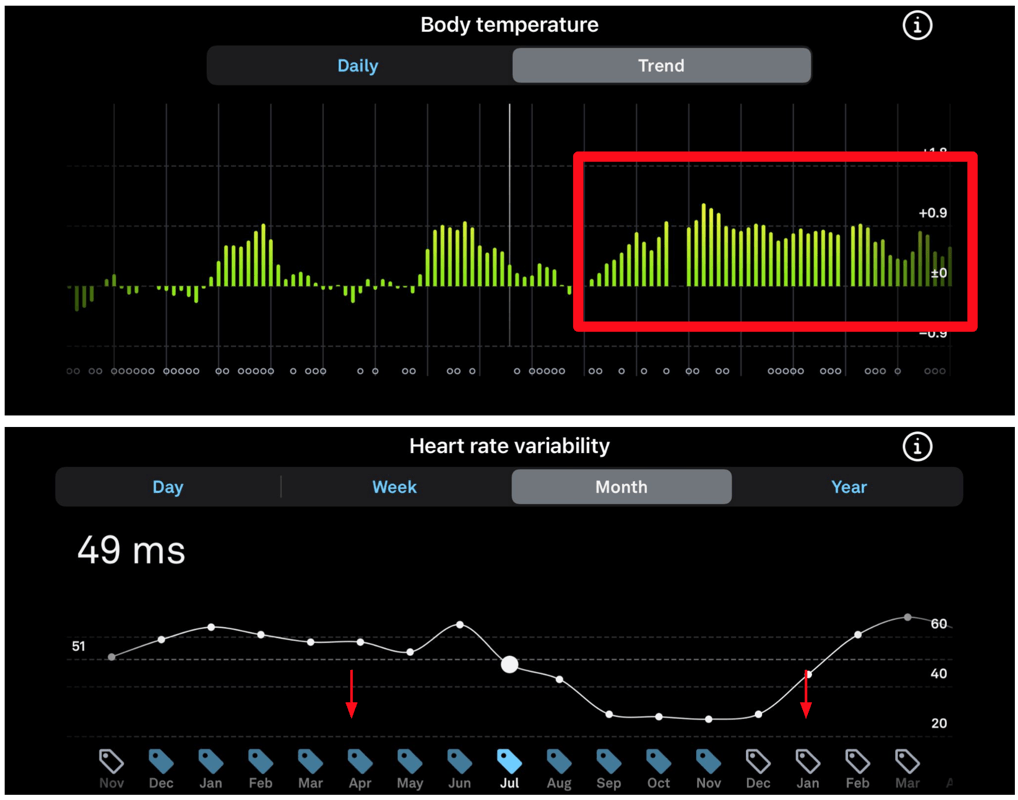
Three colleagues from the industry shared their stories with DHTs during their pregnancy and motherhood journeys. Brinnae Bent, a digital health data scientist, used a wearable device to detect and track her pregnancy. In the beginning, she noted an increase in her nightly body temperature. She also observed her heart rate variability (HRV) decrease significantly. Though these data all describe natural physiological processes, at the time, the wearable-connected app didn’t have a way of recognizing the state of pregnancy. As such, according to the app, Brinnae had a 281-day long menstrual cycle! Since that time, the wearable device manufacturer added these features to the app, and it is now better suited to address these different physiological states.
Erkuden Goikoetxea, a medical device innovation lead, also used wearable devices to track her activity levels and sleep during pregnancy. Due to the natural changes in physiology and behaviors, the overall calculated scores – that often create a fun gamified experience for the users of the DHTs – were decreasing. These insights and calculations fit for the “regular user” were in reality, not fit for a pregnant woman. The feedback was useless and discouraged her from using the wearable. Moreover, after giving birth, her sleep was still very much disrupted, resulting in even “worse” sleep scores in the app. Imagine what this can do to the mental health of a new mother!
Emily (Kunka) Lewis, a digital health innovator, experienced gestational diabetes (GD) during her pregnancy and used continuous glucose monitoring (CGM) to inform her about when she needed to administer insulin. In GD, the recommended glucose level ranges are different than for Type I or II diabetes (DM) patients. Without manual programming, Emily’s device and app automatically defaulted to the recommended glucose ranges for DM. Thankfully she uncovered this important difference in discussions with her diabetes educator and corrected the thresholds manually. However, a user without this knowledge may have kept the default glucose ranges, resulting in an increased risk of erroneous self-dosing decisions with an insulin pen in the absence of an automated closed-loop system with a connected insulin pump.
Women’s experience is not only fertility
Though there have been many stories similar to these above, pregnancy and motherhood are not the only aspects of women’s lives that can benefit from more thoughts on the inclusive development of tools. Another great example is menopause. Unlike pregnancy, it is less well described, understood, and measured. It is a multi-year transition to a later – and different – stage of women’s health, similar to puberty being a transition from childhood to adulthood. “It is also a physiological state of change that will result in new baselines and new normal,” explains Jeanne Chung, entrepreneur, and founder of Mighty Menopause. In this new normal, women should be educated to focus on more long-term health factors such as bone health, cognitive function, or heart health.
Since menopause can be defined as this transition, digital tools offer a fantastic opportunity to track the delta between “before” and “after.” High-resolution longitudinal data can help define the baselines, the changes happening over time, and also the new levels for each person. Indeed these specific tools need to be highly personalized due to the very individual nature of the changes. This offers a thin balance to strike – on one hand, the data can help researchers and clinicians define the target ranges for women in perimenopause and menopause in general, and on the other hand, they can result in new tools for better support and navigation through these changes for each specific individual.
Despite emerging initiatives in women-centric design, they have been mostly reduced to reproductive health. But women are much more than their reproductive cycle. Mansi Gupta, a women-centric innovation strategist, pointed out great examples from health, finance, wellness or retail, where creators should ask specific questions targeting the female part of their population to avoid biases often baked into our everyday thinking. In the health space, there are differences for females in every therapeutic area that need to be taken into consideration – read this article about differences between men’s and women’s hearts, for example. Moreover, many mental health issues are underdiagnosed in women, such as ADHD or autism. Examples from the finance world could be gender pay gaps (yes, still exist), lower purchasing power, or pension funds not taking into account specific twists and turns of women’s lives and careers.
What can we do better?
Recall Emily’s story with gestational diabetes – she attributes this unfortunate patient experience to a lack of timely patient education and poor design of the app’s onboarding process. Based on that, she believes that companion apps for medical devices like CGMs should employ at least some branching logic to understand and, subsequently, better tailor the user experience in a way that is “foolproof” for users with varied levels of both health and digital literacy.
A better onboarding process pinpoints a great example of possible enhancements for digital products. Here are a few more obvious improvements that can be made to the design of these tools to make them more inclusive of women’s specific needs and experiences:
- Ability to indicate clinical and physiological states and/or conditions specific to women (stage of the cycle, desired pregnancy, actual pregnancy, high-risk pregnancy, breastfeeding, pregnancy loss, perimenopause, menopause, endometriosis, etc)
- Personalization of insights or ability to hide insights completely
- Ability to input custom values or ranges
- Finding a balance in features between rigidity needed for the app to deliver value and parts that can be customized
- Including feedback loops in features and exploring when they didn’t deliver the intended value to the user
Some of the more advanced ways how to make the apps and tools more inclusive, not only in digital health products, could be:
- Adapting and personalizing algorithms that would be tailored to a specific population
- Including tailored and specific in-app education for the users
- Evaluating where designing in an intended gender neutral way ends up in biases and design fitted for male population only. What are some unintended consequences for women (or other groups) we are creating with the intention of (gender) neutral design?
- Rethinking success metrics – how can success be defined for specific groups of users?
- Exploring what resonates with women specifically in design and user experience
Moving towards change in bigger framework
Tools and algorithms created for the general population often don’t take into account specific needs and states of various subgroups, whether they are smaller or bigger. But diversity, equity, and inclusion (DE&I) is not only about race, gender, disability, or access – think again about pregnancy, age (pediatric or geriatric), people after injury, neurodiversity, etcetera. We can be safe to assume that each of these has seen some form of unmet needs within the digital health sphere.
Including these groups, such as women, in the development process is vital but not enough. We can always assume that the products are probably already biased in some way. Therefore it is important for the representatives of these respective groups (such as these several brave women here) to come forward, share their stories and make their voice heard. Each individual story counts and resonates. This will eventually create enough awareness to reach the creators and decision makers to make them pause and consider improving their products.
This pull can also benefit mainstream and non-health apps and tools and make them better. Many apps are now providing insights based on large datasets from millions of users. For these, inclusive data collection should be at the forefront during the whole product lifecycle. A call to action for developers is to re-evaluate how they approach the data collection and whether that is inclusive toward their end-user population. It ismportant to evaluate the metadata and tags (for example, demographics, socioeconomic, etc.) that can add relevant and valuable depth and context to the final algorithms and whole products.
Acknowledging these specific populations in already existing products will allow us to look at longitudinal health and wellness data that can eventually serve as baselines for future research, personalization, and improvements. For example, if pre-menopause women start using the tracking and monitoring tools now, they will have a great foundation to pinpoint and better evaluate changes when their perimenopause and menopause come. This can be tied to better health and care insights and, eventually, better outcomes for the individuals.
Some of the final remarks from our conversation might be the following -inclusivity in data collection that informs and/or creates the product, listening to use-case stories, learning about and looking for biases, personalize what’s possible, having great UX and success metrics, and always strive to make your products better and more inclusive. The individual nature of every single person is beautiful, and we are on the best path towards making the best experience tailored to everyone’s specific life story and needs.

